Blank Patient Demographics Form
Key takeaways
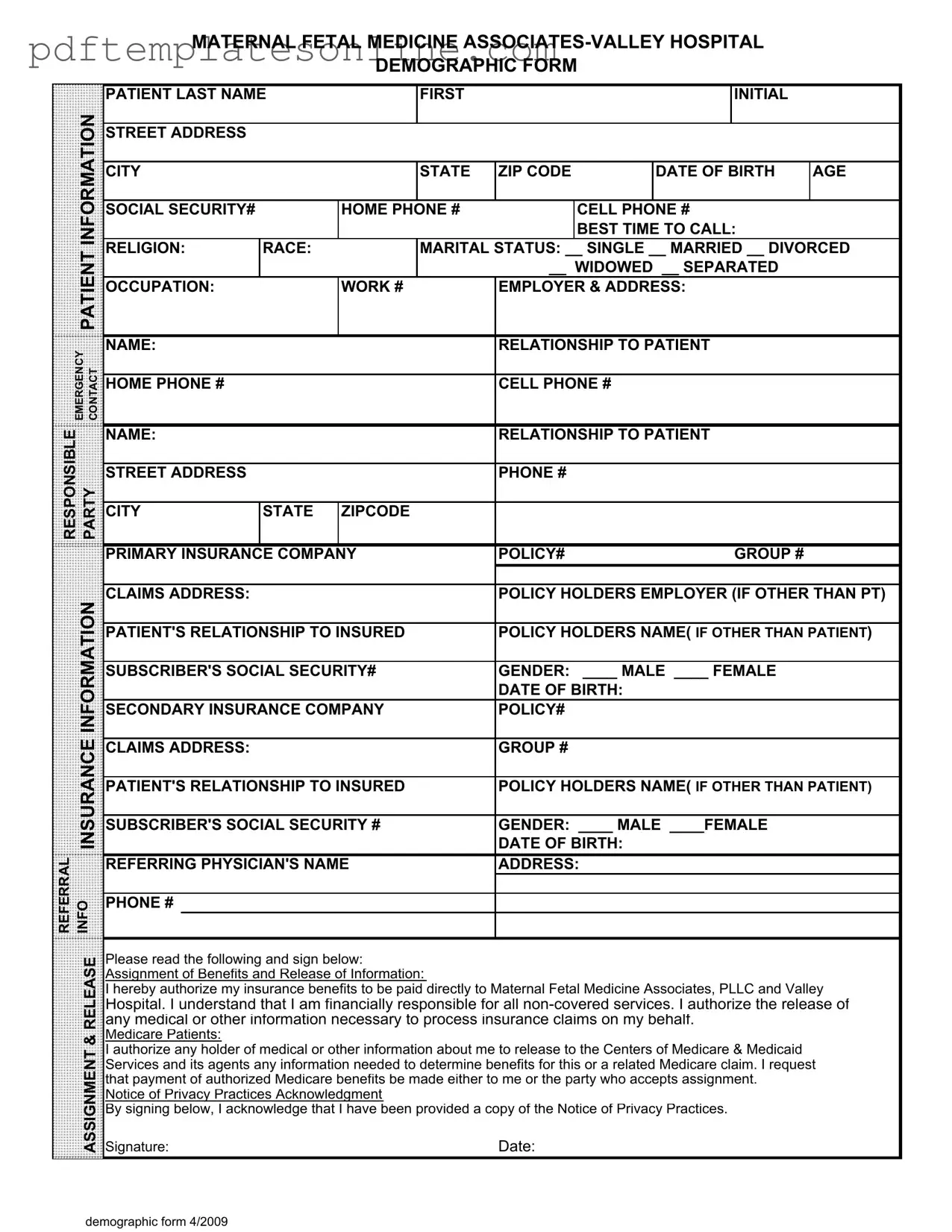
Here are key takeaways for filling out and using the Patient Demographics form:
- Provide accurate personal information, including your full name, address, and date of birth.
- List your contact numbers, including home and cell phone numbers, and indicate the best time to reach you.
- Include your social security number for identification purposes.
- Specify your marital status by checking the appropriate box.
- Enter details about your occupation and employer, including the employer's address.
- Designate an emergency contact, providing their name, relationship to you, and their contact numbers.
- Complete insurance information, including primary and secondary insurance details, policy numbers, and claims addresses.
- Indicate your gender and provide the date of birth for both yourself and any insured parties.
- Read and understand the Assignment of Benefits and Release of Information section before signing.
- Sign the form to acknowledge receipt of the Notice of Privacy Practices.
Common mistakes
Completing the Patient Demographics form accurately is crucial for ensuring that healthcare providers can deliver the best possible care. However, many individuals make common mistakes that can lead to delays or complications in their medical treatment. Here are nine frequent errors to avoid when filling out this important document.
One common mistake is omitting the social security number. This information is often necessary for insurance processing and can lead to delays if not provided. Always double-check that this field is filled in correctly to avoid unnecessary complications.
Another frequent oversight is leaving out the emergency contact information. It is vital to have someone listed who can be reached in case of an emergency. Ensure that the name, relationship, and phone numbers are accurate and up to date.
Many people also forget to indicate their marital status. This information can sometimes impact insurance coverage and billing. Take a moment to carefully select the appropriate option, whether you are single, married, divorced, widowed, or separated.
In addition, individuals often neglect to provide complete insurance information. Ensure that both primary and secondary insurance details are filled out thoroughly. Missing policy numbers or claims addresses can delay the processing of claims and lead to unexpected out-of-pocket expenses.
Another common error is not specifying the best time to call. This information helps the office reach you at a convenient time, making communication smoother. Be sure to indicate when you are most available to receive calls.
People sometimes fail to provide their occupation and employer information. This data can be important for understanding your medical history and potential work-related health issues. Always include this information accurately.
Additionally, some patients mistakenly leave the race and religion fields blank. While these may seem optional, they can be relevant for demographic studies and patient care considerations. Filling them out can help healthcare providers better understand and cater to your needs.
Another oversight is not signing the release of information section. This signature is crucial for allowing your healthcare provider to communicate with your insurance company. Without it, your claims may be delayed or denied.
Finally, many individuals overlook the importance of reading the Notice of Privacy Practices. Acknowledging that you have received this document is essential for understanding how your personal information will be used and protected. Always take the time to read and sign this acknowledgment.
By being mindful of these common mistakes, you can help ensure that your Patient Demographics form is filled out correctly, facilitating a smoother healthcare experience.
Misconceptions
- Misconception 1: The Patient Demographics form is optional.
- Misconception 2: All information on the form is shared with the public.
- Misconception 3: Only insurance information is collected.
- Misconception 4: The form is only for new patients.
- Misconception 5: Completing the form takes too much time.
- Misconception 6: Providing demographic information is not important.
- Misconception 7: The form does not require accurate information.
- Misconception 8: The form is only for administrative purposes.
- Misconception 9: I can refuse to provide my Social Security number.
In reality, completing this form is often mandatory for healthcare providers to ensure accurate patient records and billing.
Patient information is protected under privacy laws, such as HIPAA, which restricts unauthorized access and sharing.
The form gathers various details, including personal, demographic, and emergency contact information, not just insurance data.
Even returning patients may need to update their information to reflect any changes since their last visit.
While it may seem lengthy, most patients can complete it in a matter of minutes, especially with prepared information.
This information is crucial for healthcare providers to deliver appropriate care and understand patient populations.
Providing accurate information is essential for effective communication and proper billing processes.
While it serves administrative functions, the data collected also helps in clinical decision-making and patient care.
While you can refuse, not providing it may complicate insurance claims and processing, potentially delaying care.
Dos and Don'ts
When filling out the Patient Demographics form, it’s important to ensure accuracy and completeness. Here’s a list of things you should and shouldn't do:
- Do provide your full last name and first initial.
- Do include your complete street address, city, state, and ZIP code.
- Do enter your date of birth accurately.
- Do include a reliable home phone number and cell phone number.
- Do specify your best time to call.
- Don't leave any required fields blank.
- Don't use nicknames or abbreviations for your name.
- Don't forget to provide emergency contact information.
- Don't omit details about your insurance coverage.
- Don't sign the form without reading the release and acknowledgment statements.
Other PDF Forms
Final Waiver of Lien Chicago Title - It provides assurance that the project has been completed according to agreed terms and conditions.
In the realm of financial agreements, understanding the importance of a well-structured Loan Agreement is crucial, as it lays the foundation for the lending relationship. To facilitate this process, you can access the necessary documentation, like the comprehensive California Loan Agreement form, through resources such as California PDF Forms, which provide templates that ensure clarity and protection for both the lender and borrower.
Quest Lab Requisition Form - Test preferences can vary by physician and patient needs.
Yugioh Deck List Sheet - Document the round for context related to the infractions listed.
Detailed Guide for Writing Patient Demographics
Completing the Patient Demographics form is an essential step in ensuring that your healthcare provider has accurate and up-to-date information. This information will help facilitate your care and ensure that all necessary communications and insurance claims are handled efficiently. Below are the steps to fill out the form accurately.
- Patient Last Name: Write your last name in the designated space.
- First Initial: Enter your first initial next to your last name.
- Street Address: Fill in your complete street address.
- City: Indicate the city where you reside.
- State: Select your state from the dropdown or list provided.
- ZIP Code: Input your ZIP code.
- Date of Birth: Write your date of birth in the specified format.
- Age: Enter your current age.
- Social Security Number: Fill in your Social Security number.
- Home Phone Number: Provide your home phone number.
- Cell Phone Number: Enter your cell phone number.
- Best Time to Call: Specify the best time for the office to reach you.
- Patient Religion: Indicate your religion.
- Race: Fill in your race.
- Marital Status: Select your marital status by checking the appropriate box.
- Occupation: Write your current occupation.
- Work Number: Provide your work phone number.
- Employer & Address: Fill in the name and address of your employer.
- Emergency Contact Name: Enter the name of your emergency contact.
- Relationship to Patient: Specify your relationship to the emergency contact.
- Emergency Contact Home Phone: Provide the home phone number of your emergency contact.
- Emergency Contact Cell Phone: Enter the cell phone number of your emergency contact.
- Responsible Party Name: Fill in the name of the person responsible for your bills.
- Relationship to Patient: Specify your relationship to the responsible party.
- Responsible Party Street Address: Enter the street address of the responsible party.
- Responsible Party Phone Number: Provide the phone number of the responsible party.
- City: Fill in the city of the responsible party.
- State: Indicate the state of the responsible party.
- ZIP Code: Enter the ZIP code of the responsible party.
- Primary Insurance Company: Write the name of your primary insurance company.
- Policy Number: Fill in your insurance policy number.
- Group Number: Enter your group number.
- Claims Address: Provide the claims address for your insurance.
- Policy Holder's Employer: If different from the patient, write the employer's name.
- Patient's Relationship to Insured: Specify your relationship to the insured.
- Policy Holder's Name: Fill in the name of the policy holder if different from you.
- Subscriber's Social Security Number: Enter the Social Security number of the subscriber.
- Gender: Check the appropriate box for your gender.
- Date of Birth: Write the date of birth for the policy holder.
- Secondary Insurance Company: If applicable, provide the name of your secondary insurance.
- Policy Number: Enter the policy number for your secondary insurance.
- Insurance Claims Address: Fill in the claims address for your secondary insurance.
- Group Number: Enter the group number for your secondary insurance.
- Patient's Relationship to Insured: Specify your relationship to the insured for the secondary insurance.
- Policy Holder's Name: Write the name of the policy holder for the secondary insurance.
- Subscriber's Social Security Number: Enter the Social Security number for the secondary subscriber.
- Gender: Check the appropriate box for the secondary insured's gender.
- Referral Information: Provide the name of the referring physician.
- Address: Fill in the address of the referring physician.
- Phone Number: Enter the phone number of the referring physician.
- Release Section: Read the assignment of benefits and release of information carefully.
- Signature: Sign the form to authorize the release of information.
- Date: Write the date you are signing the form.
- Notice of Privacy Practices Acknowledgment: Sign below to acknowledge receipt of the privacy practices notice.